BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV)
BPPV is the most common of the vestibular disorders. It is experienced by 2.4% of all people at some point during their lifetime.
If enough otoconia become dislodged from their normal position in the utricle, they will aggregate and migrate to the lowest portion of the semicircular canal (usually posterior). The otoconia may still move when the head changes position, causing one to feel as if the head and body are spinning or the world is spinning.
Sometimes, a direct cause for the dislodging of the otoconia can be identified, such as head trauma, rough motions of the head, labyrinthine conditions, Meniere's disease or vestibular migraines. However, the cause is not known for all vestibular disorders.
Sub-types of the disorder can be identified based on the semicircular affected and if the otoconia are free floating (canalithiasis) or attached to the cupula (cupulothiasis).
If enough otoconia become dislodged from their normal position in the utricle, they will aggregate and migrate to the lowest portion of the semicircular canal (usually posterior). The otoconia may still move when the head changes position, causing one to feel as if the head and body are spinning or the world is spinning.
Sometimes, a direct cause for the dislodging of the otoconia can be identified, such as head trauma, rough motions of the head, labyrinthine conditions, Meniere's disease or vestibular migraines. However, the cause is not known for all vestibular disorders.
Sub-types of the disorder can be identified based on the semicircular affected and if the otoconia are free floating (canalithiasis) or attached to the cupula (cupulothiasis).
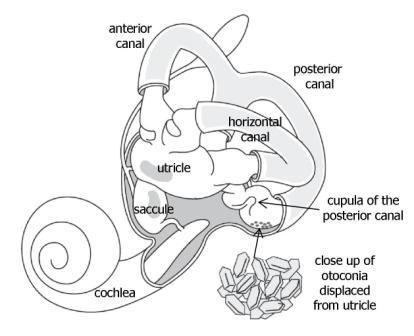
Otoconia from the utricle may become lodged in the semicircular canals, leading to the feeling of spinning associated with BPPV.
Symptoms
While benign, symptoms of BPPV may hit suddenly and without warning. However, changes in the position of the head will also induce symptom attacks. As the posterior semicircular canal is most commonly affected, the most problematic head movements tend to include looking up and getting out of bed.
In addition to vertigo, sufferers of BPPV may also experience dizziness, imbalance, and nausea. These symptoms may come and go or last a lifetime, depending on the patient and the treatment administered.
In addition to vertigo, sufferers of BPPV may also experience dizziness, imbalance, and nausea. These symptoms may come and go or last a lifetime, depending on the patient and the treatment administered.
Diagnosis
Diagnosis of BPPV will usual occur following physical examination, conducting vestibular and auditory tests, and completing lab work to rule out other diagnoses.
The Dix-Hallpike maneuver and the supine roll test can both be used as tests for BPPV. During these tests, doctors will watch for nystagmus. Nystagymus, seen below, is an involuntary jerking of the eyes that accompanies head movement. It is caused by a failure in communication in the vestibular-ocular reflex. These tests can be performed in conjucntion with Frenzel goggles to magnify the nystagmus, allowing easier diagnosis of the condition.
The Dix-Hallpike maneuver and the supine roll test can both be used as tests for BPPV. During these tests, doctors will watch for nystagmus. Nystagymus, seen below, is an involuntary jerking of the eyes that accompanies head movement. It is caused by a failure in communication in the vestibular-ocular reflex. These tests can be performed in conjucntion with Frenzel goggles to magnify the nystagmus, allowing easier diagnosis of the condition.
Treatment
In most cases, a simple in-office treatment can be used to remove the otoconia from the semicicular canal. The Epley maneuver, illustrated below, is a series of movements of the patients head designed to remove the otoconia from the semicircular canal. In 20-30% of patients, symptoms recur within the first week and the maneuver must be repeated. In the long term, BPPV recurs about half of the time. In rare cases, such as when the canal is blocked by the otoconia, surgery may be performed in rare cases surgery must be performed to remove the otoconia.
"About Vestibular Disorders." Vestibular Disorders. Johns Hopkins Medicine. Web. 25 Nov. 2013. <http://www.hopkinsmedicine.org/neurology_neurosurgery/specialty_areas/vestibular/>.
Lee, Steve (2012). "Benign Paroxysmal Positional Vertigo." Retrieved November 24, 2013. emedicine.medscape.com.
Vestibular Disorders Association. Web. 25 Nov. 2013. <http://vestibular.org/>.
Lee, Steve (2012). "Benign Paroxysmal Positional Vertigo." Retrieved November 24, 2013. emedicine.medscape.com.
Vestibular Disorders Association. Web. 25 Nov. 2013. <http://vestibular.org/>.
